CCDA Information
Component Overview
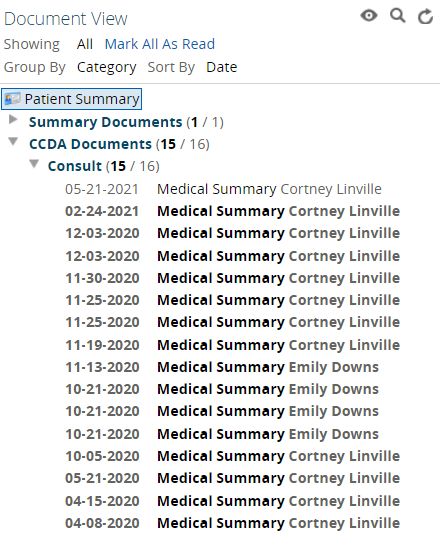
For participating organizations that submit clinical data on their patients through Consolidated Clinical Document Architecture (CCDA) formatted data sets, this information will not be included within the “Patient Summary” view. Instead, it will flow to a separate folder titled “CCDA Documents” within the “Document View” component. This component is located along the left-hand side of the "Patient Summary" view.
Key Functionality
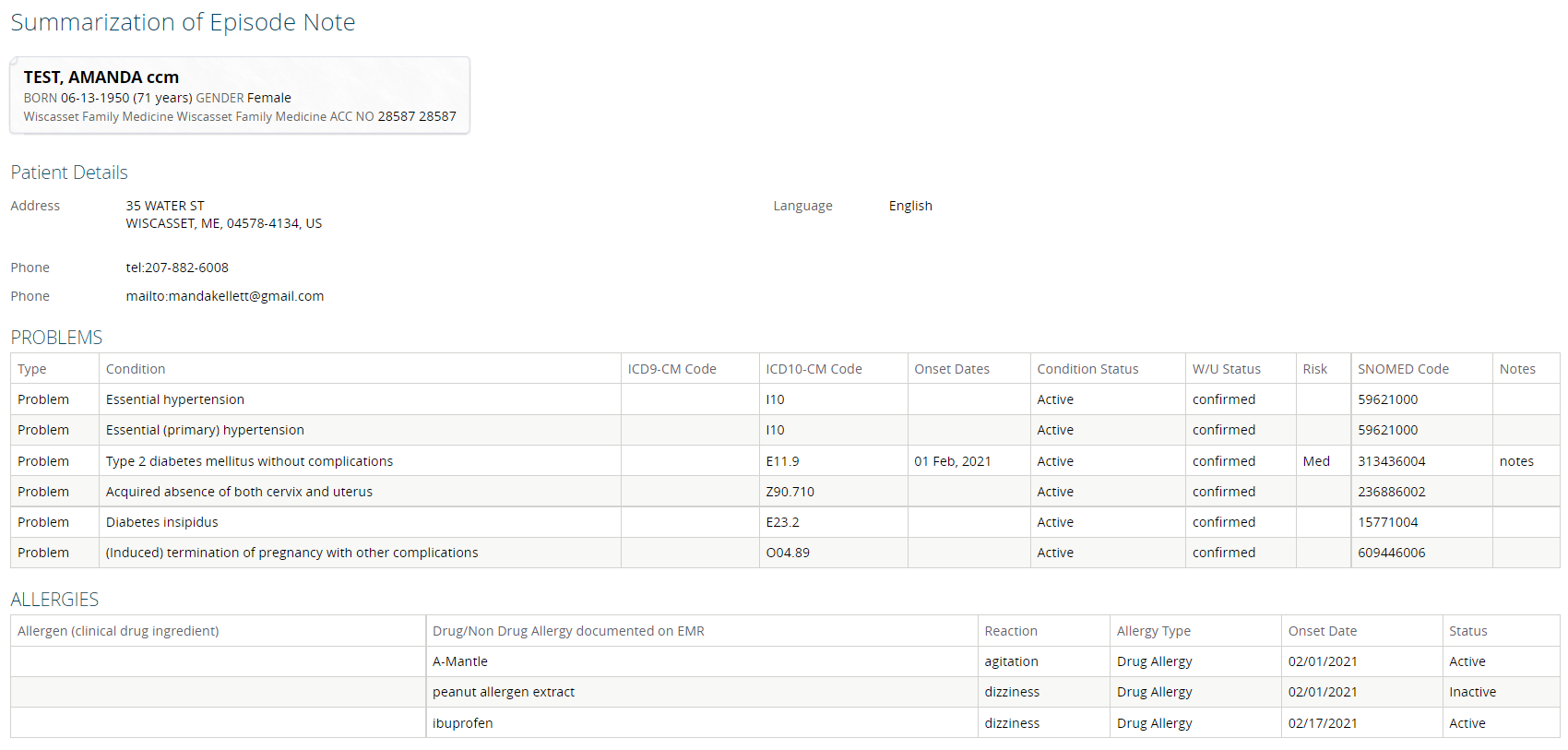
Since CCDA information is not currently parsed into discrete data elements within the Clinical Portal, all clinical information received on patients from participating providers sending data in the CCDA format will be included in the selected record from the “Document View”; the information will not exist anywhere else within the patient’s “Patient Summary” view.
The CCDA standard is an Extensible Markup Language (XML) document summarizing current and pertinent historical information about a patient’s healthcare activity at a given facility. Although not every document type contains every section, the current CCDA standard supports the following information: Allergies, Care Team, Encounter History, Hospital Discharge Instructions (inpatient visits only), Functional/Cognitive Status, Immunizations, Instructions, Medications, Patient Demographic Details, Plan of Care, Problems/Encounter Diagnoses, Procedures, Reason for Hospitalization (inpatient visits only), Reason for Referral, Reason for Visit (ambulatory visits only), Results, Social History, Vital Signs.